| �Indicate Format Needed ~ Place "X" in box | ||||
| PC41-NJ Format 1 (MD, DO, DS, DMD, DPM, DVM)
Imprint up to 4 Names
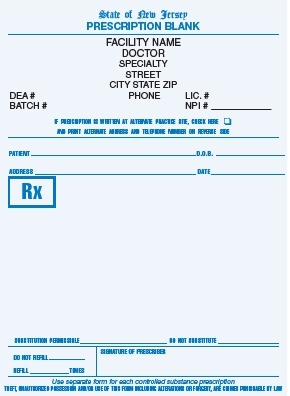 click to enlarge |
PC42-NJ Format 2 (Facility Format)
Imprint the Facility Name, Address and Phone Number.
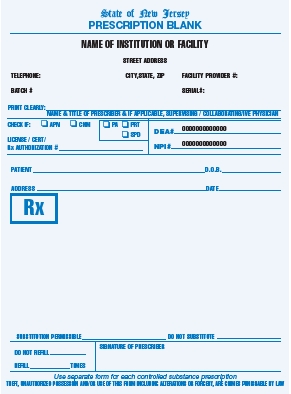 click to enlarge |
PC43-NJ Format 3 (Optician Format) �
Imprint maximum 4 Names or 3 Names plus Facility Name.
 click to enlarge |
PC44-NJ Format 4 (Nurse Practitioner) New Jersey law requires only ONE Nurse Practitioner's name per script with ONE Collaborative Physician's name. Both the Nurse Practitioner's name and information plus the Collaborative Physician's name and information must be pre-printed on script.
 click to enlarge |
PC48-NJ Format 5 (Physician Assistant) New Jersey law requires only ONE Physician Assistant's name per script with ONE Collaborative Physician's name. Both the Physician Assistant's name and information plus the Collaborative Physician's name and information must be pre-printed on script.
 click to enlarge |